Fallserie




















































































Chirurgisches Management von Wirbelsäulentumoren (Bukarest 2023)
55 Folien
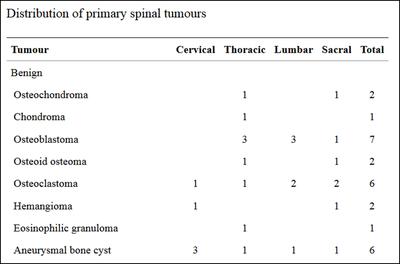
Spinal tumors
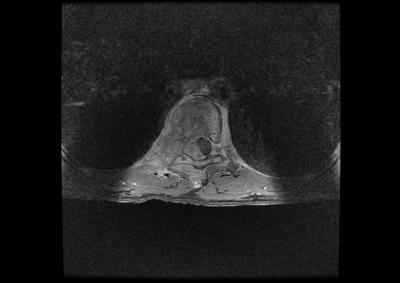
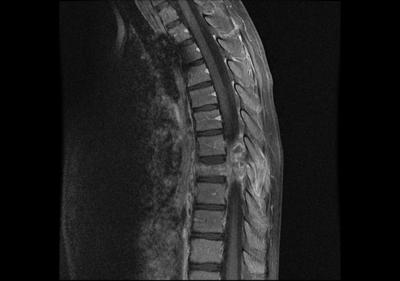
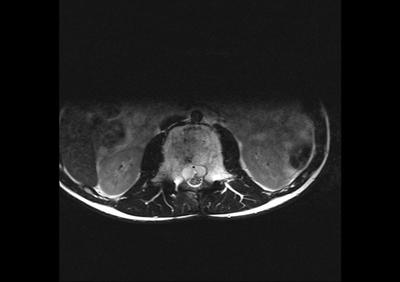
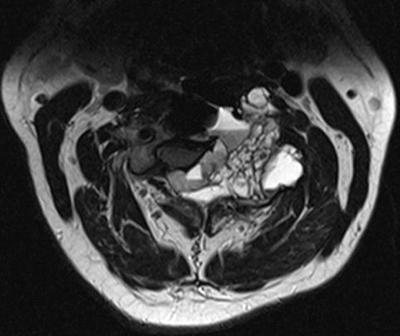
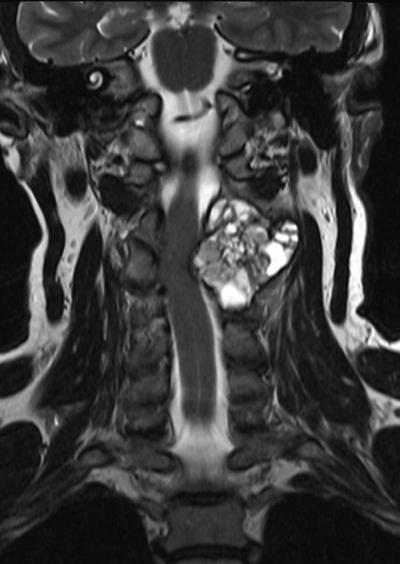
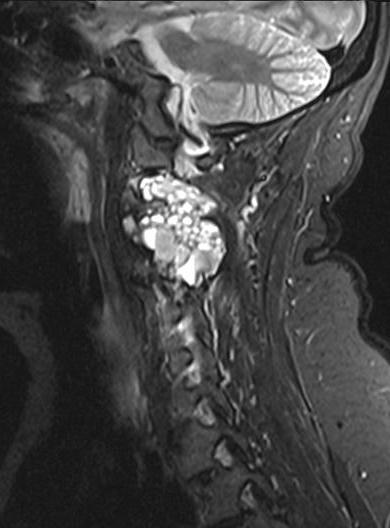
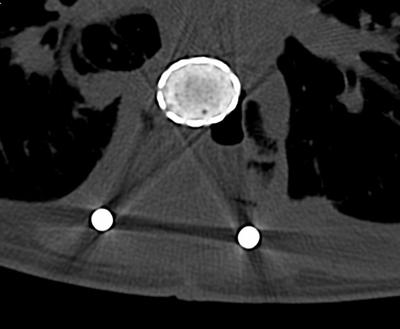
Benign - Osteoblastoma
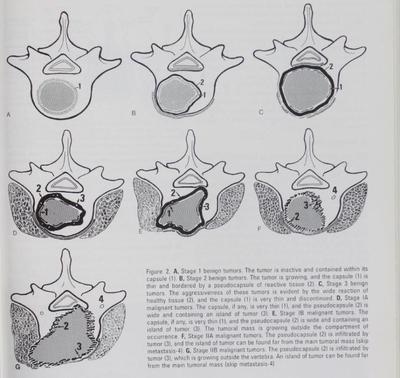
Benign bone tumors
S1(latent), S2 (active), S3 (agressive)
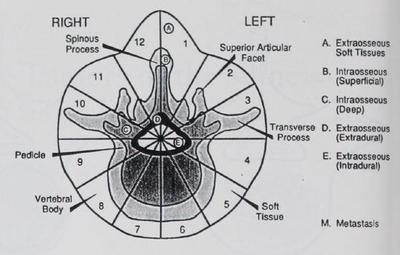
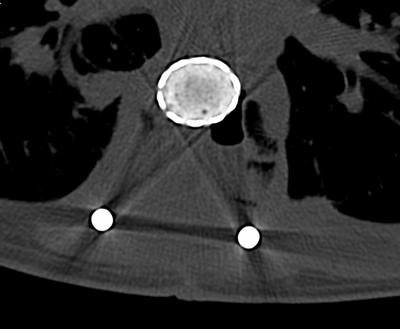
Vertebral body divided in 12 quadrants and 5 „rings“from paravertebral to dural
Biopsy mandatory
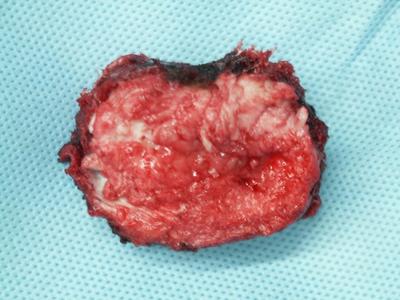
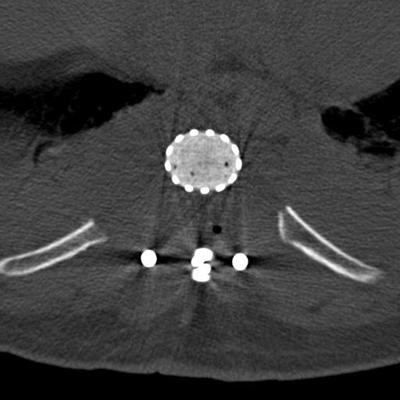
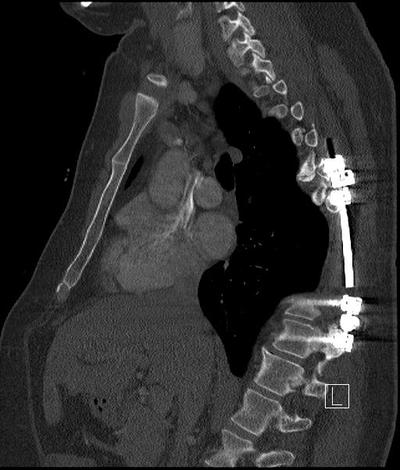
Total En-bloc Vertebrectomy / Spinal Reconstruction
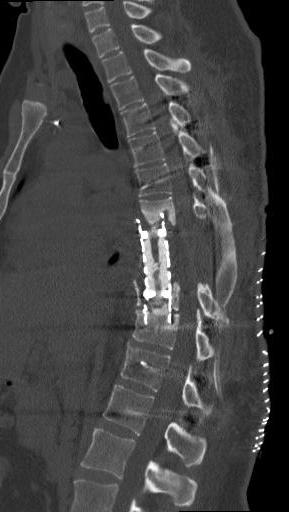
Total en bloc spondylectomy - TES
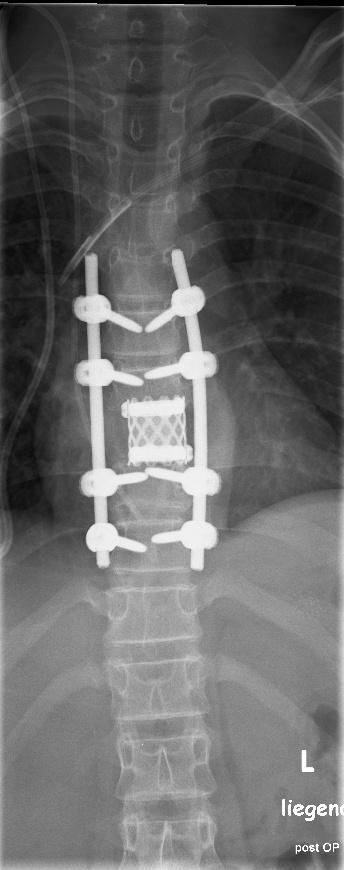
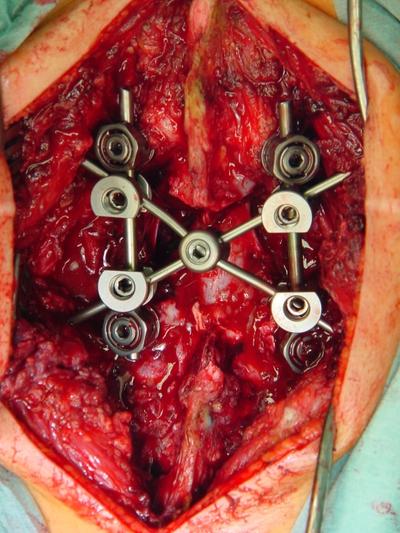
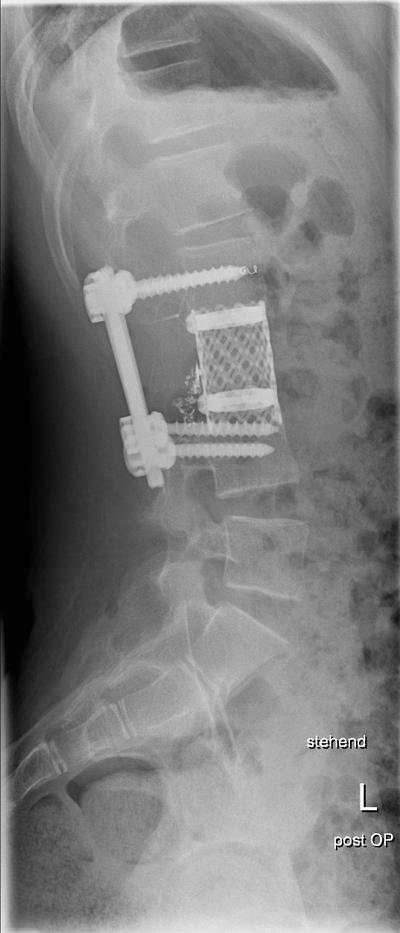
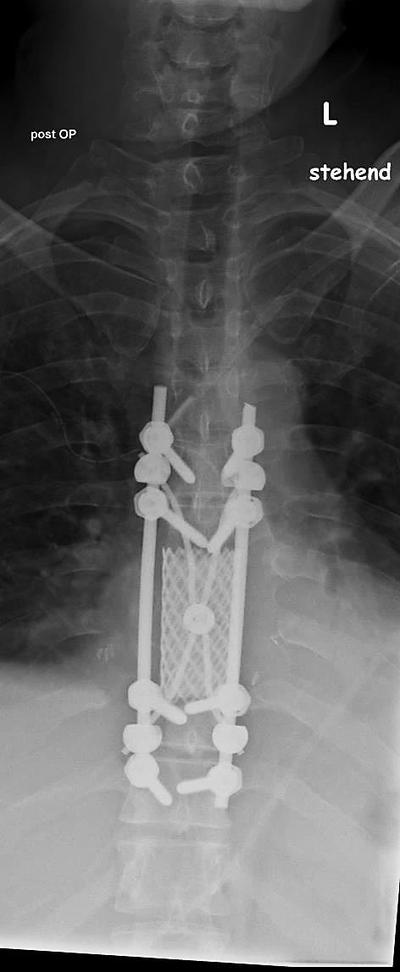
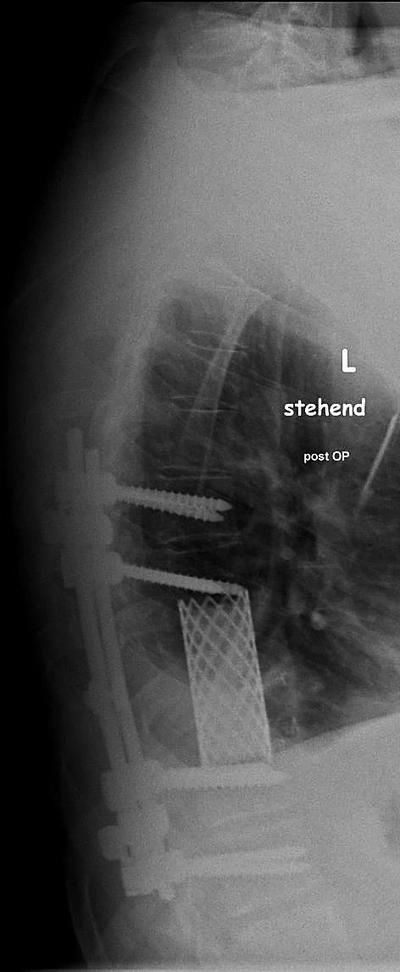
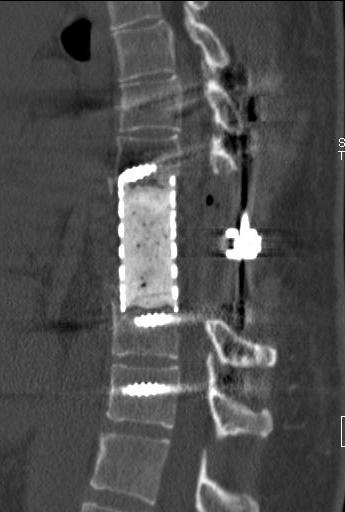
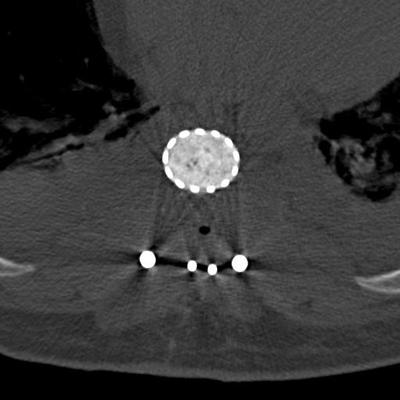
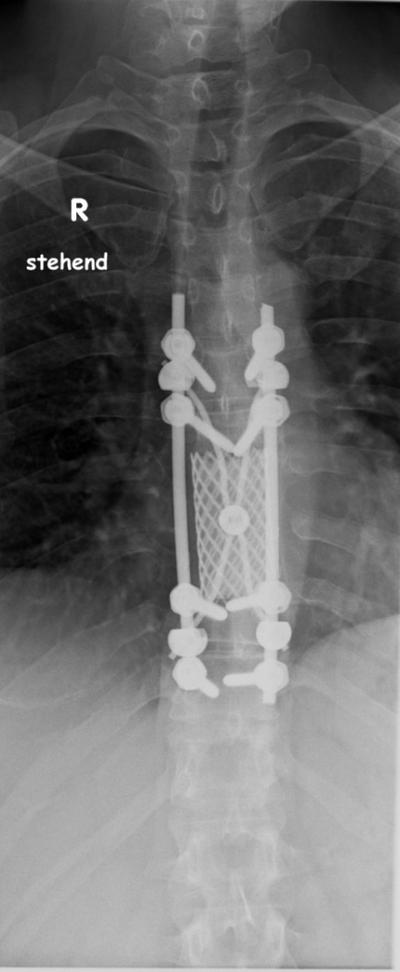
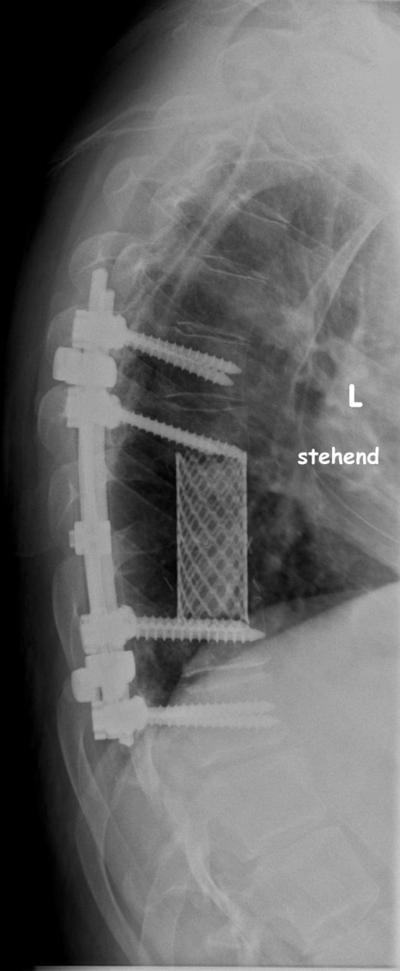
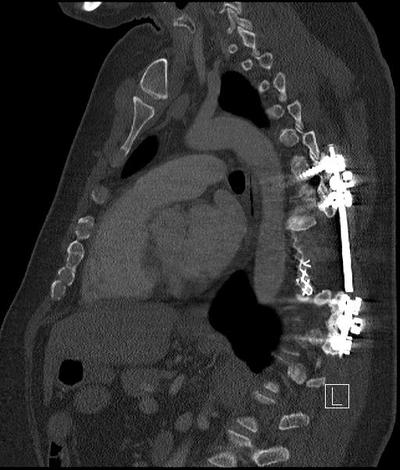
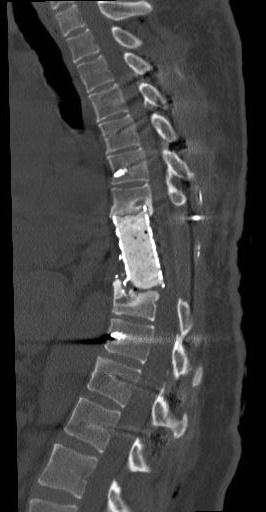
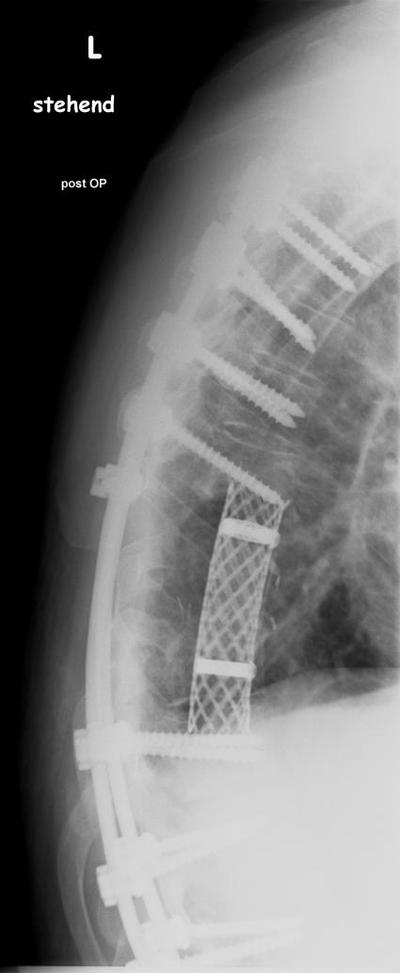
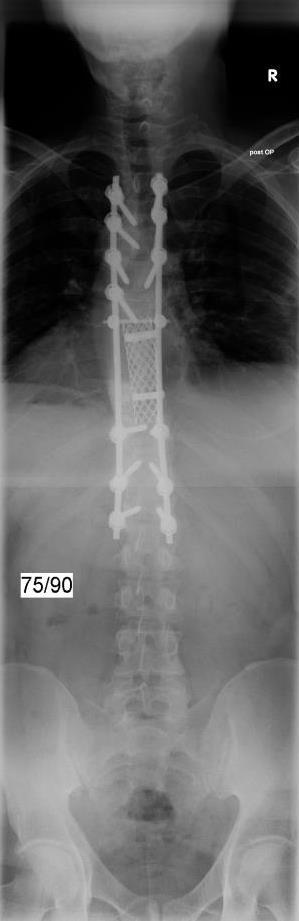
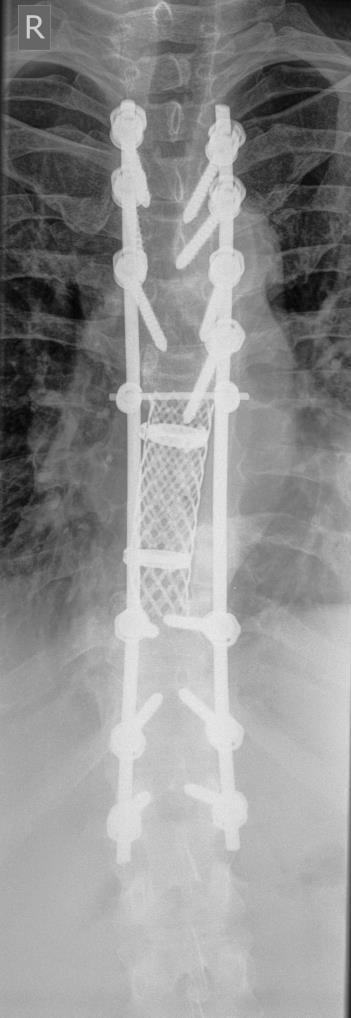
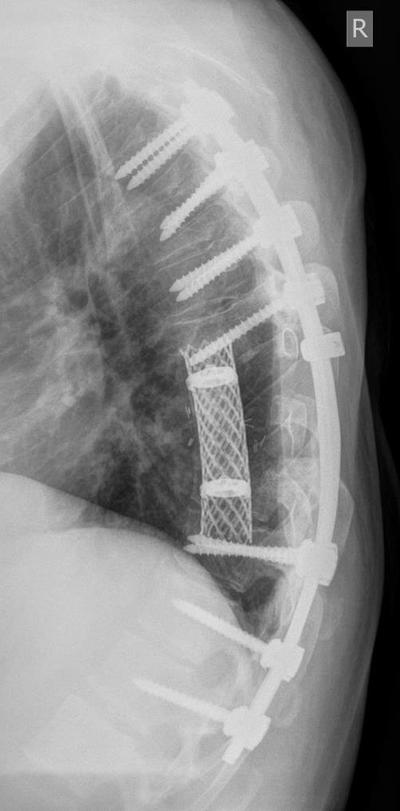
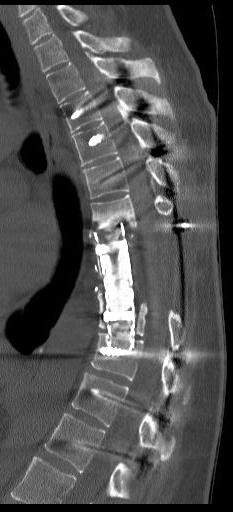
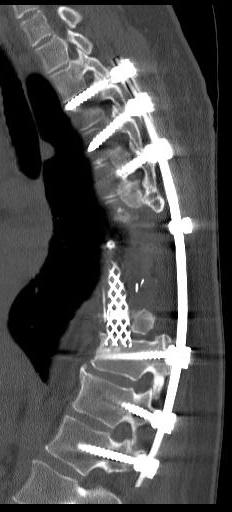
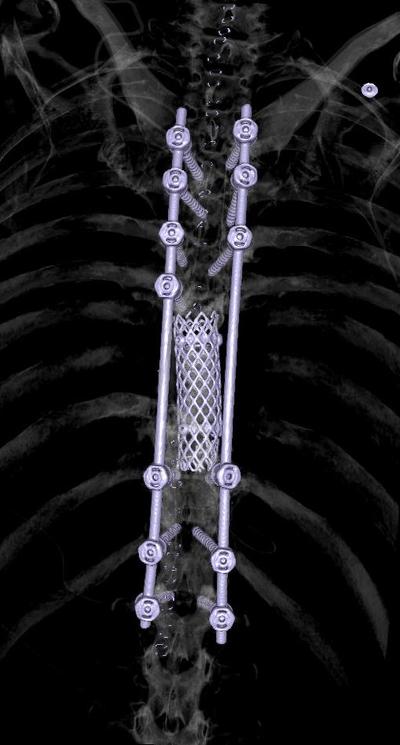
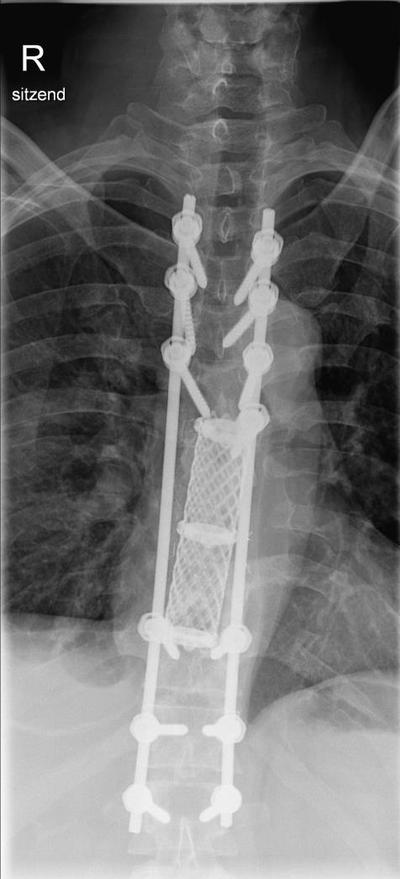
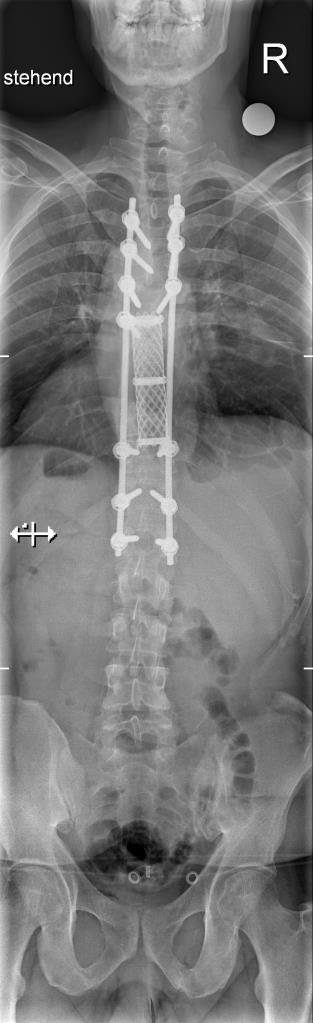
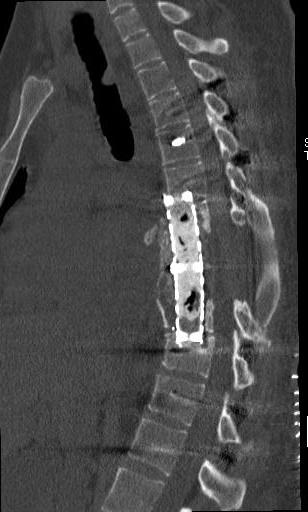
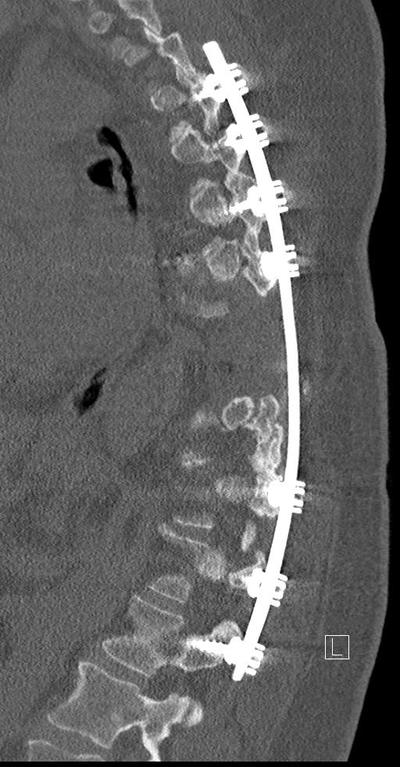
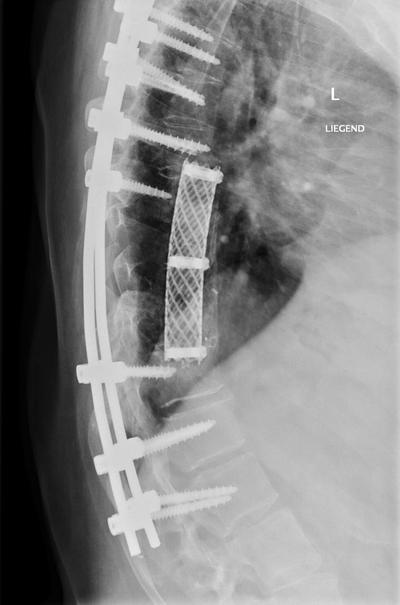
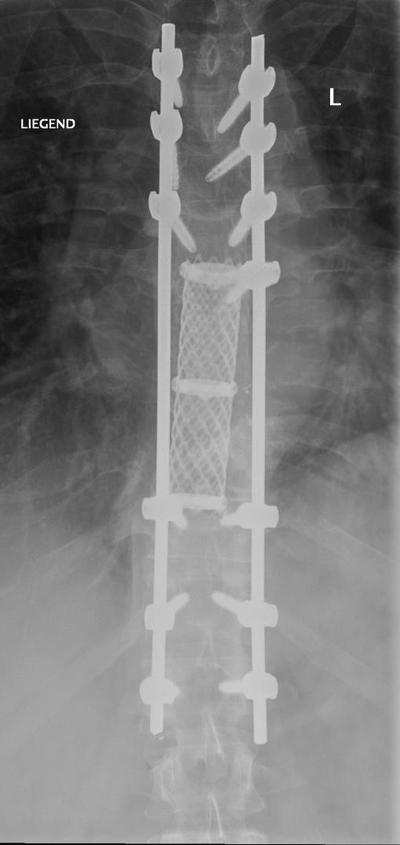
Spinal Reconstruction
Spinal Reconstruction
Spinal Reconstruction
Spinal Reconstruction
Spinal Reconstruction
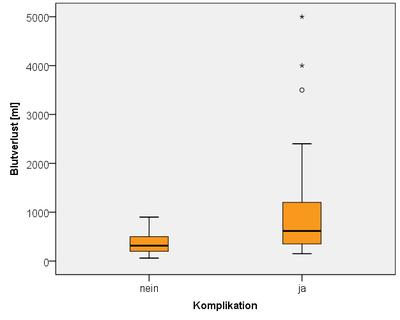
24 cases of total en bloc spondylectomy between 6/2011 - 6/2014, 5 surgeons
Results and Complications
Seite 23
Single metastasis in mamma carcinoma
Single metastasis in mamma carcinoma, extracavitary en bloc resection
31,M, Chondrosarcoma
61, M, Chordoma
16, m, Ewing sarcoma
13, M, Haemangioma
17, M, aneurysmat. bonecyst
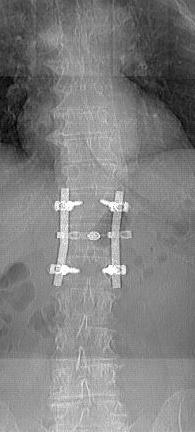
09/2006
01/2007
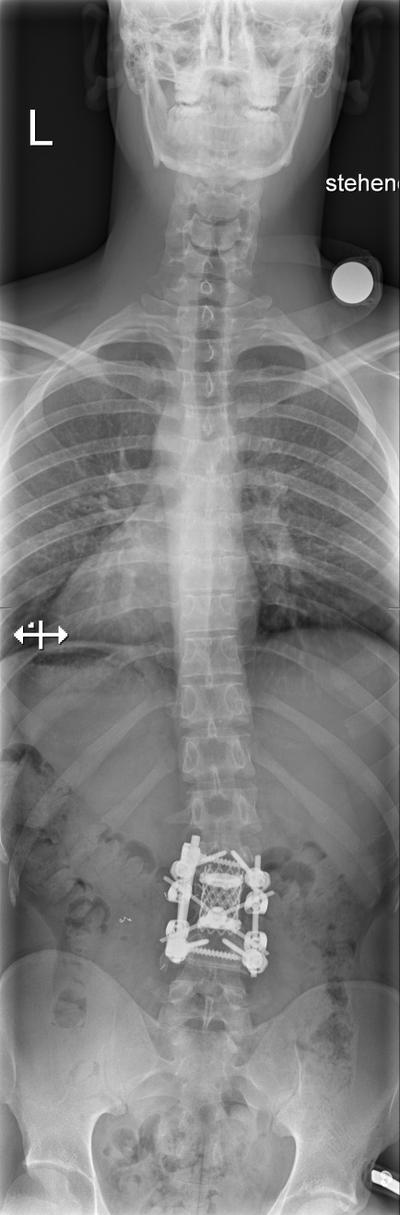
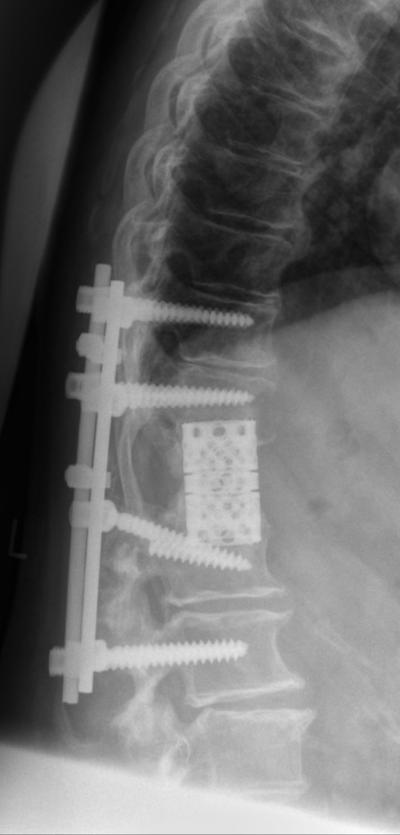
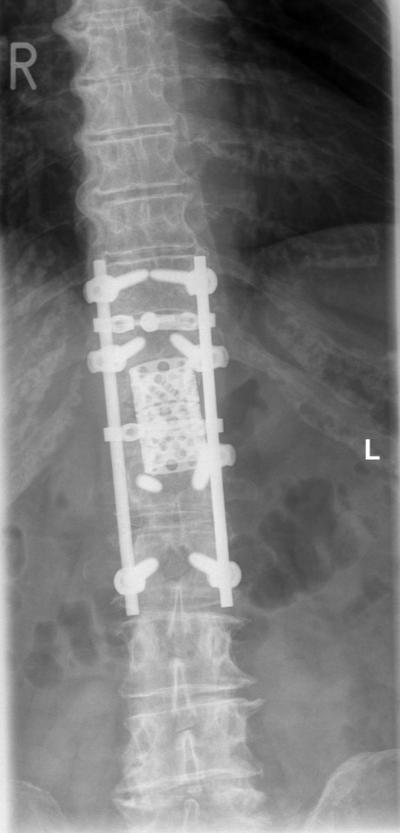
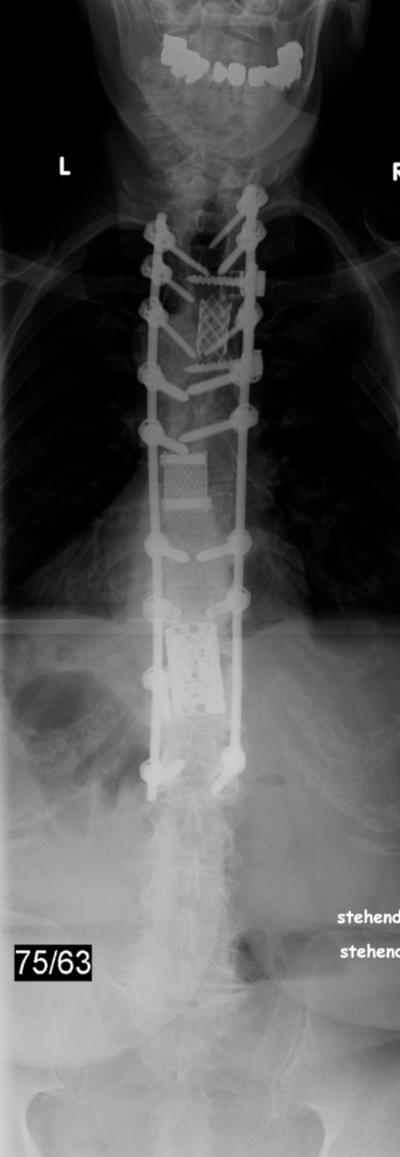
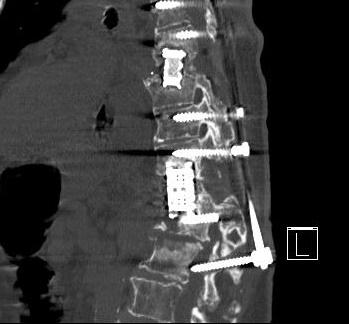
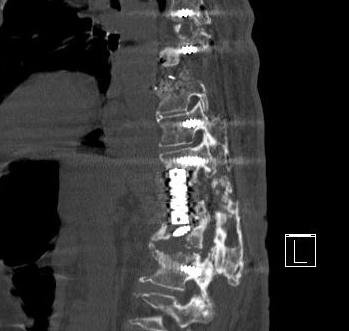
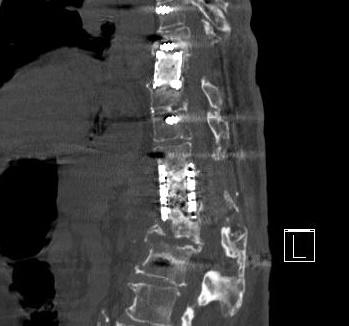
Spinal Reconstruction
11/2011
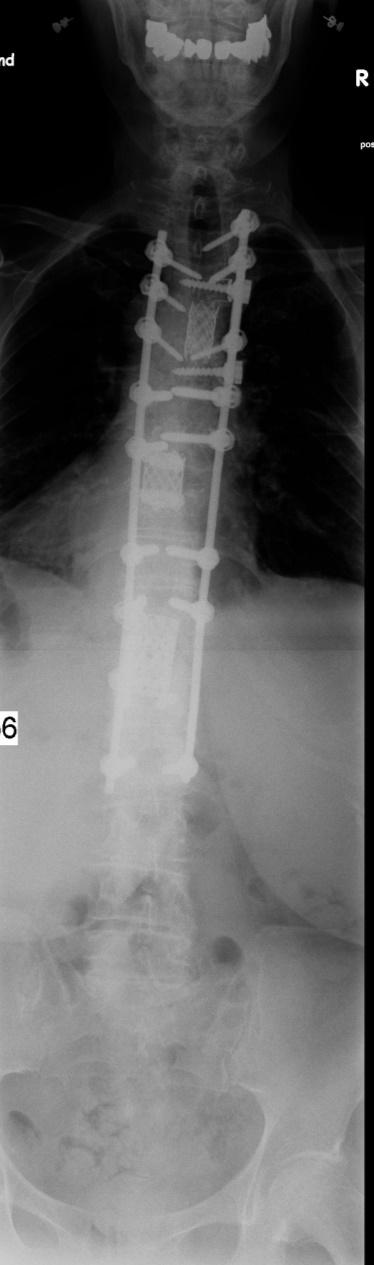
10/2014: posterior revision, instrumentation to L5
Case2:
12/2006
02/2011
10/2011
10/2011
03/2012
12/2012
12/2012
12/2012
06/2017
08/2017
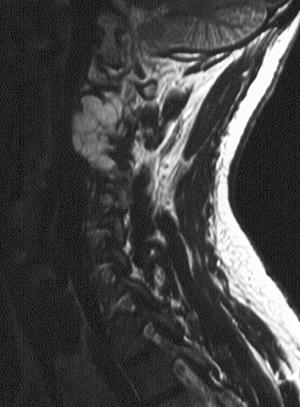
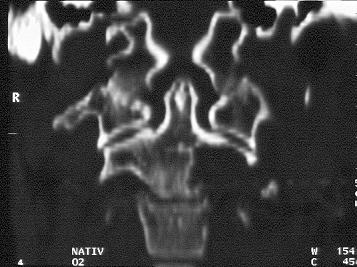
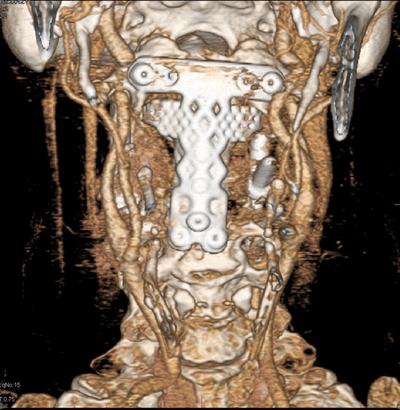
Case 3: 54y, f.
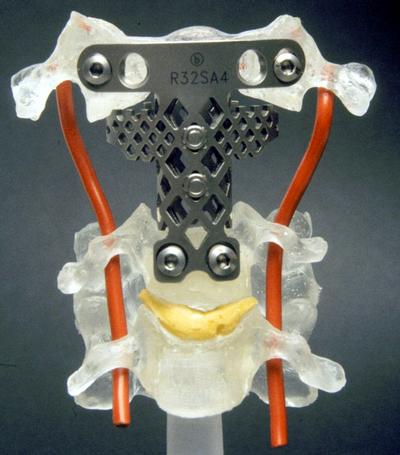
Combined approach (transoral with mandibula/ tongue split, anterior high cervical, posterior):
06/2016
Spinal Reconstruction